


How to Identify and Treat Hypergranulation Tissue
-
 Susan Dieter MS, RN, CWS
Susan Dieter MS, RN, CWS
- January 28, 2021
 Excessive granulation tissue is often referred to as hypergranulation, overgranulation, exuberant tissue or proud flesh. It is a condition in which fibroblast and new capillary growth is excessive, resulting in a raised appearance above the wound margins. Hypergranulation tissue must be addressed as it prevents epithelialization and wound healing.
Excessive granulation tissue is often referred to as hypergranulation, overgranulation, exuberant tissue or proud flesh. It is a condition in which fibroblast and new capillary growth is excessive, resulting in a raised appearance above the wound margins. Hypergranulation tissue must be addressed as it prevents epithelialization and wound healing.
What is normal granulation?
Normal granulation tissue demonstrates an elevated cellular density, incorporating a collection of fibroblasts, macrophages, and new vessels in a randomly-organized collagen matrix that forms at the base of open wounds. It incorporates a dense network of blood vessels – newly growing capillaries (in a process known as angiogenesis) with an irregular upper layer creased by the capillaries looping together on the wound surface. This gives granulation the appearance of red lumps (or granules) within the normal paler pink matrix, and despite this pink to red appearance, granulation does not bleed easily. Once the wound is filled with granulation tissue, it provides a foundation for re-epithelialization.
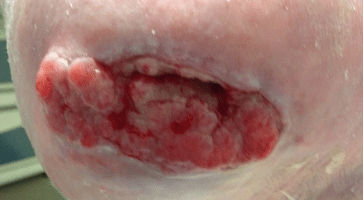
What is hypergranulation?
Hypergranulation is excessive granulation that rises above the wound surface, imposing a barrier to the inward-migrating epidermis. Certain areas — such as the scalp, temples, and lower leg — are prone to forming hypergranulation tissue. It is recognized by a friable red to dark red, often shiny and soft appearance, which is raised to the level of the surrounding skin or higher. This tissue must be removed in order for re-epithelialization to occur.
What causes hypergranulation?
The exact cause of hypergranulation is unknown, but it is often linked with infection, pressure or friction to the wound bed, negative pressure suction (particularly when using large pore foam) and a cellular imbalance related to the underlying patient pathology. ¹

How do you treat hypergranulation?
Treatments for hypergranulation tissue reported in the literature are based on elimination of the causative factor. They focus on reducing bioburden, applying compression, decreasing the occlusiveness of the dressings selected, physical removal and the use of steroid therapy.
A high bioburden is postulated to alter the local environment of the wound, resulting in further lowering of the oxygen tension and accounting for the finding of increased neovascular formation around the foci of wound infection. The hypergranulation tissue typically associated with high bioburden and infection is a brown-red color with a loose friable surface that bleeds easily. Surgical debridement of the hypergranulated tissue and appropriate control of infection and/or wound bioburden with an antimicrobial wound cleanser and/or dressing may be utilized for treatment. ²,³
What is the role of chronic wound fluid in emphasizing hypergranulation?
Irritation caused by chronic wound fluid in contact with the wound bed or persistent pressure/friction is another cause of hypergranulation tissue. This may include wound dressings or treatments that typically impact an initial inflammatory response for healing and may result in increased exudate. Proactively managing that temporary increase in exudate will aid in preventing hypergranulation tissue. Hypergranulation tissue that is caused by chronic exudate or pressure/friction can be addressed with surgical removal of the hypergranulation tissue and application of the appropriate topical dressing to contain exudate, such as a foam dressing and wound off-loading. ⁴ The foam dressing manages the excess exudate and offloading decreases pressure/friction to the wound bed.
Steroid impregnated tapes containing fludroxycortide may also be considered. Treatment with 1% hydrocortisone cream is another steroid application that may be used. As with other topical steroids, the therapeutic effect is primarily the result of its anti-inflammatory and antimitotic mode of action.
 Is cauterization an effective treatment for hypergranulation?
Is cauterization an effective treatment for hypergranulation?
Occasionally, cautery with silver nitrate may be used to treat hypergranulation, but it is cautioned as it can be painful for the patient and caustic to healthy granulation tissue. The cauterization to the hypergranulated surface will necrose the superficial granulation tissue, which can then be wiped off.⁵ The use of silver nitrate directly reduces fibroblast proliferation and is therefore not recommended for prolonged or excessive use. This technique should only be used if all else has been ineffective.
What is the difference between malignancy and hypergranulation?
 Note that malignancy in a wound may be mistaken for hypergranulation. Suspect a malignant transformation when over-granulation is irregular, hard to touch, exceeds the edges of the wound (cauliflower or ‘stuck on’ appearance), does not respond to treatment and has months of evolution. If there is any doubt, a biopsy should be performed.
Note that malignancy in a wound may be mistaken for hypergranulation. Suspect a malignant transformation when over-granulation is irregular, hard to touch, exceeds the edges of the wound (cauliflower or ‘stuck on’ appearance), does not respond to treatment and has months of evolution. If there is any doubt, a biopsy should be performed.
Care in treating and determining the underlying cause for challenges in wound healing, along with provision of a supportive wound environment, are keys to successful wound management.
Visit Sanaramedtech.com for more information regarding wound care and wound care products.
References
- Vandeputte J and Hoekstra H. Overserved hypergranulation may be related to edema of granulation tissue. (2006)
- Browne A, Dow G and Sibbald RG. Infected wounds: definitions and controversies. In Falanga V, Cutaneous Wound Healing. Martin Dunitz (2001), 204.
- Stephen-Haynes. Managing Overgranulation. Wound Care Today. (2013); 1-21.
- Vuoloo J. Hypergranulation: exploring possible management options. British Journal of Nursing (2010):19(6):S4-S8.
- Dealy C. The Care of Wounds, 2nd Edition. 1999.